|
Surgical treatment
A wide variety of approaches to repairing the injured AC joint have been proposed. Most shoulder specialists nowadays agree that incomplete dislocations, i.e. those known as Tossy I and II injuries, do not need to be treated surgically at first. An operation may be needed at a later date, but more for the treatment of AC arthrosis resulting from the dislocation than for the treatment of the AC instability.
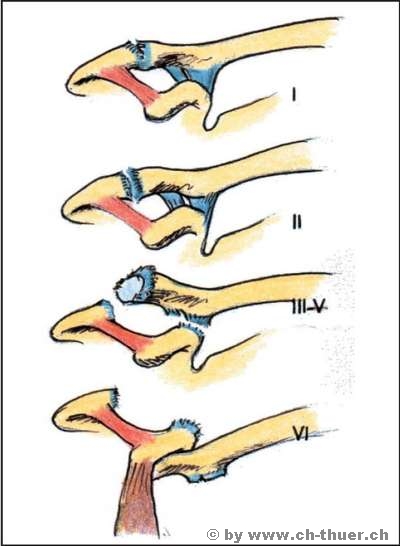
Complete dislocations with complete separation of the suspensory apparatus (Tossy III injuries, i.e. Rockwood 4-6) should be reconstructed provided the patient can be offered a good reconstruction technique with the prospect of a good outcome.
As you may notice from my comments above, specialists are not of one mind as how to manage this type of injury. Of course, no-one likes the sensation of a complete and often troublesome misalignment in the AC joint. Any surgeon would naturally want to try and restore the integrity of the joint. To be honest, though, reconstructions rarely produce an ideal outcome.
A powerful meniscus is located between the end of the collarbone and the acromion, and this is usually torn in AC dislocations.
Full joint integrity can therefore be restored only if the meniscus remains intact. If it has been torn, it will need to be surgically removed and, however good the restoration of joint congruity and the ligaments, arthrosis will still subsequently develop in the AC joint. This wearing down of the joint by the joint surfaces rubbing against each other leads, over time, to painful arthrosis, which in turn relativises the result of the AC joint reconstruction, particularly as a pain-free result can often be achieved without surgery.
In view of these considerations, I have found the following procedure to be effective:
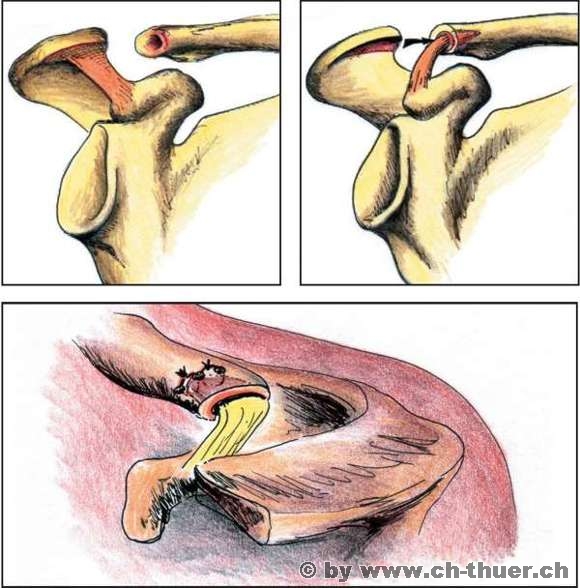
In cases of complete AC dislocation, reconstruction with preservation of the intact meniscus should be attempted. If this is not possible because the meniscus is torn, I reconstruct the suspensory structure of the shoulder by transferring a strong adjacent and uninjured ligament, removing the injured meniscus and extending the AC joint so that the two joint surfaces are no longer able to rub against each other.
A modified version of this method according to Weaver-Dunn (the first person to describe this technique) is shown in the drawings below. With very few exceptions the results are very good, and patients are generally completely satisfied and able to resume sporting activities.
|