|
Treatment
The dislocated shoulder should be reduced as soon as possible, but without using force.
Various methods have been described and recommended. Most important of all is the need for gentle and careful reduction so as to avoid causing any additional structural injury during the reduction manoeuvre. Although the joint does not necessarily need to be immobilised after reduction, it is recommended until the pain subsides, which usually takes 3-7 days.
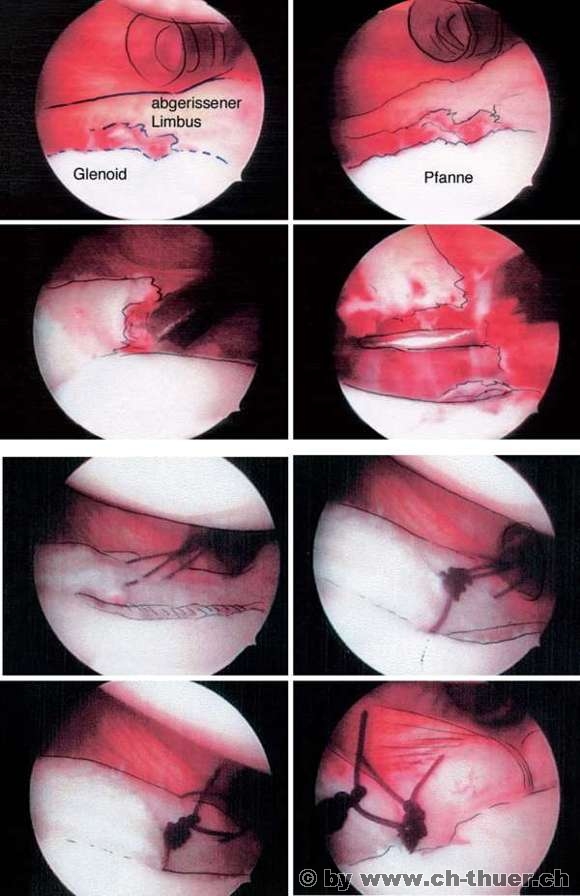
Repeated post-traumatic shoulder dislocations require surgical correction. Now that it is possible to use arthroscopy to manage these injuries and achieve very good outcomes, a number of surgeons and orthopaedists have adopted the practice of surgically treating first-time dislocations in young patients in order to avoid any extension of the joint damage in the event of repeat dislocation.
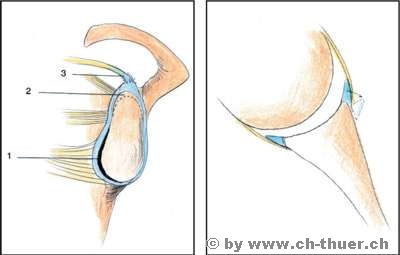
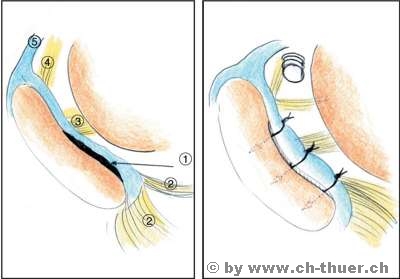
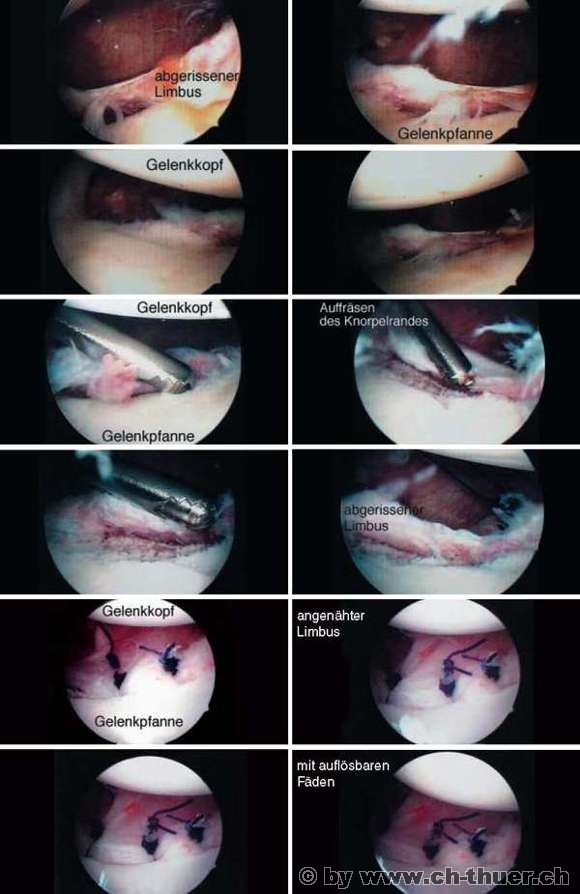
During the arthroscopic procedure, the torn meniscus and torn ligaments can be reattached to the anterior edge of the joint. This procedure spares the surrounding soft tissues and enables surgeons to rebuild the injured structures using dissolvable materials (absorbable sutures) so that the joint can be returned to its original state once the reconstruction has healed.
In some cases, however, open surgery will still be required, particularly for more extended injuries and repeated dislocations after a previous arthroscopic procedure.
|