|
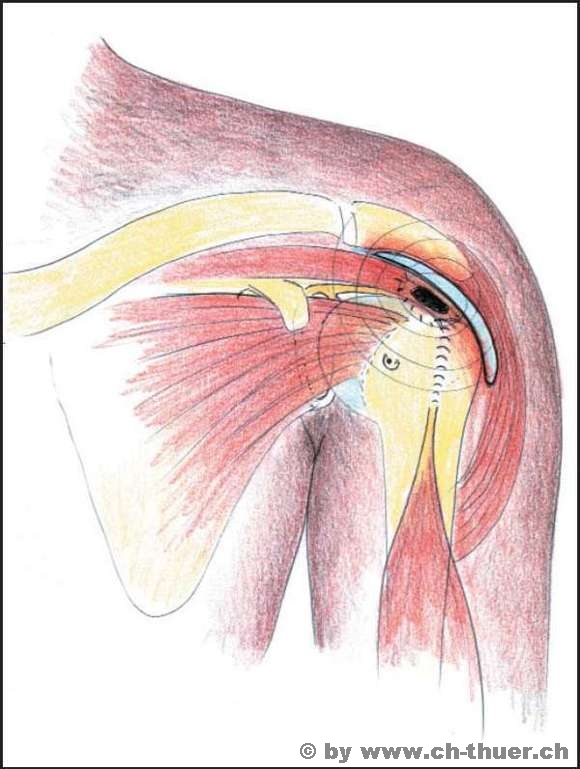
Rotator cuff impingement syndrome occurs in three stages.
In stage I there is no definite damage as a result of tissue constriction, just swelling accompanied by fluid accumulation in the tissue. The treatment at this stage consists of rest, anti-inflammatory medication and treatments, application of cold, physiotherapy to strengthen the centring muscles, etc.
Stage II is characterised by sustained constriction and impingement of the tissues with initial chafing of the rotator cuff, partial lesions, tissue hardening.
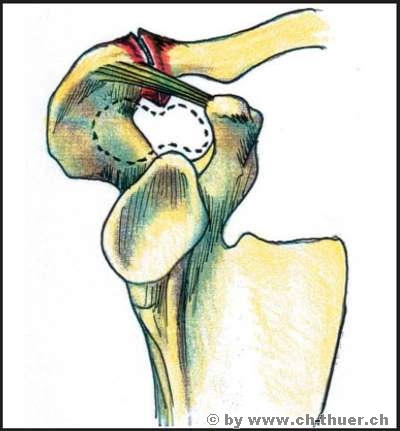
In stage III we then see the established damage, with destruction of the bursa and tear lesions on the RC. Stages two and three have to be surgically treated. The tissue beneath the acromion has to be relieved and the roof widened, either to produce a wedge shape or in the form of a lift-up osteotomy of the acromion. The bursa is removed.
But in addition to these roof-widening and space-creating measures, the causes of the constriction in particular must be eliminated, e.g. RC reconstruction for tears, correction of constricting fracture fragments from humeral head injuries, restoration of the centring function in the shoulder.
|